
China's Vaccines? Yeah, They "Kinda" Work.
August 6, 2021

As we head into H2 2021 and continue our oil thesis, we’re keeping focus on the global economic recovery and Delta. Delta’s recent spread around the world has recently become a headwind, and its severity largely depends on where you live.
For countries in developed markets (“DMs”) with high vaccination rates and efficacious vaccines, we’ve begun to see a decoupling between the number of positive cases and deaths, which is further evidence that the vaccines are working. Perhaps not as well at preventing infection in the new Delta variant, but still highly efficacious in protecting against severe illnesses and death, and so long as we don’t overwhelm our hospitals, deaths shouldn’t inflect from lack of care.
US
In the US, there’s good news and bad news. The bad news is that positive cases are likely much higher than currently shown. Given the higher transmissibility of the Delta variant, we believe COVID cases are likely double what’s being reported for the simple fact that we’re not testing as much as we were in the prior waves.

In fact, we’re testing about 1.5x less than we were in the Winter/Fall, which is to say that it’s very likely that “real world” case rates are much higher because the two are correlative.
The good news is that the divergence between increasing case counts and deaths are also showing-up in the US data, again a sign that the vaccines are doing their job.

In addition, while overall hospitalizations are still increasing, the “velocity” may be peaking. As you may recall, we’ve analogized COVID spread to a wild fire, and have used “net hospitalizations” as an indicator of the severity/ferocity of that spread. We’ve long held that hospitalizations are a better indicator than positive cases because the latter varies based on the number of tests and many are asymptomatic. Also severe cases are what we’re concerned with, and if those inflect, our health care systems could become inundated, leading to reduced quality of care and higher mortality rates. Fortunately, as you can see, net hospitalizations (i.e., the pressure of hospitalizations) are beginning to plateau/decline.

If true, we should see this curve start to level off and decline, which would indicate that the Delta wave is beginning to abate.
Given that a significant portion of the US population has been vaccinated, and more importantly almost 80% of those over 65 (with 2 doses), we anticipate the figures will begin to roll-over in the coming two weeks (cases and hospitalizations). US health restrictions are at low levels today, and many locales have already unlocked, allowing the virus to spread largely unchecked. At this stage of our pandemic response, people will either develop antibodies from the vaccine or the disease itself. The only difference is your level of discomfort and risk tolerance.
Politicization of the vaccines means that it’s largely the Republican red states (with lower vaccination rates) that are bearing the disproportionate brunt of new infections. Unfortunately, those states are also populated by more people who have a comorbidity, which increases the risk of severe illness and death.

Nonetheless, this is the path of our recovery as vaccines are readily available, prevalent, and free. For better and for worse, we likely won’t lockdown (blue states won’t lock for those refusing vaccinations and red states won’t lock because, well, they never will), and if cases do tip-over then we all should have some additional immunity for the winter.
China
For emerging markets (“EMs”), Asia Pacific is also experiencing a similar rise in cases, hospitalizations and deaths, the severity of which is much higher and akin to India as those countries are largely unvaccinated due to the unavailability of vaccines. That’s changing as more deliveries make their way across the Pacific, and manufacturers/distributors now focus on EMs as DMs are now experiencing gluts of vaccines.
All eyes are also focused on China, where an outbreak in 14 of the 32 provinces has forced authorities to reinstitute local/regional lockdowns and mobility restrictions to combat the spread. Clusters in at least 26 cities across China, including Hunan, Nanjing and Beijing means the news sounds ominous. Yet, it’s important to keep in mind that we’re talking about ~600 cases. Certainly Delta’s transmissibility is a concern, but China had success containing a Delta outbreak in Guangdong earlier in June (i.e., one of the largest port cities), and will be running the same playbook countrywide.
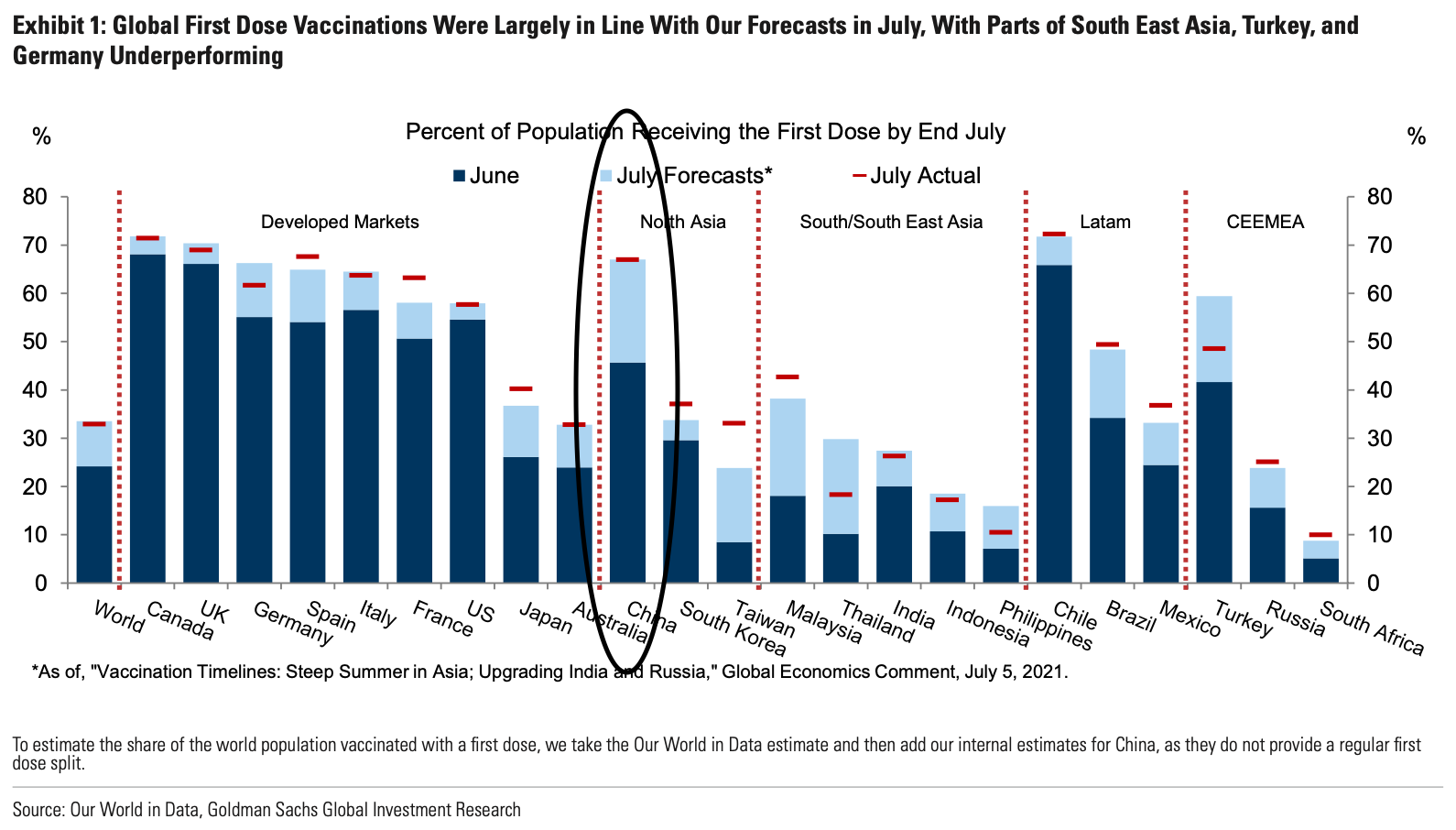
Now one could also argue that the population has some level of immunity because over 65% of its populace have already received a first dose. Ponder that for a moment. China has a population of 1.4B people (vs. 330M in the US). 1.4B. They’ve administered close to 1.7B doses already, and the country is well on its way to achieving an 80% vaccination rate by year end (if we exclude children (i.e., those under 18, and a accounting for 20% of the population), then we’ll largely have China fully vaccinated by year end.
However, there are still lingering doubts.
Made in China
Sure you jabbed over a billion doses, but do the vaccines actually work? Now that’s the key question, and the answer seems to be a resounding . . . kinda.
China is dosing itself largely with 2 vaccines, one produced by Sinovac called CoronaVac, and another made by Sinopharm. Both are inactivated vaccines that trigger the production of antibodies to fight COVID.

There’s very little data on the efficacy of Sinovac and Sinopharm vaccines on Delta, but we do have some data with Alpha (the original Wuhan variant). Sinovac claims that CoronaVac was ~66% effective against preventing COVID, ~88% preventing hospitalizations, and ~86% preventing death.

Sinopharm touted ~79% effectiveness at preventing symptomatic and hospitalized cases combined. Importantly, there were insufficient people over 60 in the clinical trials to estimate efficacy in the highest risk cohort. Even more importantly, the above efficacy rates were again for the Alpha variant and not the more transmissible Delta.
Chile - China - China - Chile
For Delta though, we can look to a real world example, Chile. As part of its vaccine diplomacy, China offered free vaccines to many countries. Chile eventually dosed 60% of its population with CoronaVac, and just this week Chilean health officials released a follow-on study of the vaccine’s efficacy. For millions of Chileans who received CoronaVac between February to July, here’s the results (including results from an earlier study released in April).
For preventing symptomatic infections, Sinovac was ~60% effective. Slightly lower than the 66% effectiveness registered in an earlier study (in April), but about the same as AstraZeneca’s (“AZ”) 69%.

If we look at hospitalizations, particularly ICU admissions, we’re seeing really robust protection, 90%, but again still trailing AZ’s 98%. If we look at AZ’s protection against Delta for these severe cases, it’s also lower, registering 71%. We’d again anticipate a slightly lower figure for Sinovac on Delta as well, though no data was presented.

Lastly for deaths, Sinovac has also proven to be lower at 86% whereas all the other vaccines offered full protection. No data yet on AZ’s efficacy for preventing deaths with Delta.

So where does that leave us? Well it’s safe to say that the Sinovac’s vaccine is effective, but ~10% lower than AZ’s shot for the earlier variants of COVID. As time passed, CoronaVac’s efficacy also declined (like most other vaccines). In addition, it’s also fair to assume that the vaccines are less effective at preventing symptomatic Delta cases, and if we assume an “AZ level” of comparability, then CoronaVac is likely also ~30% effective for Delta as well.
The above data also means that CoronaVac does provide decent protection against severe cases, and if we look at Chile’s cases to death count rates, they are performing much better than other South American countries with lower vaccination rates (see Chile on the bottom).

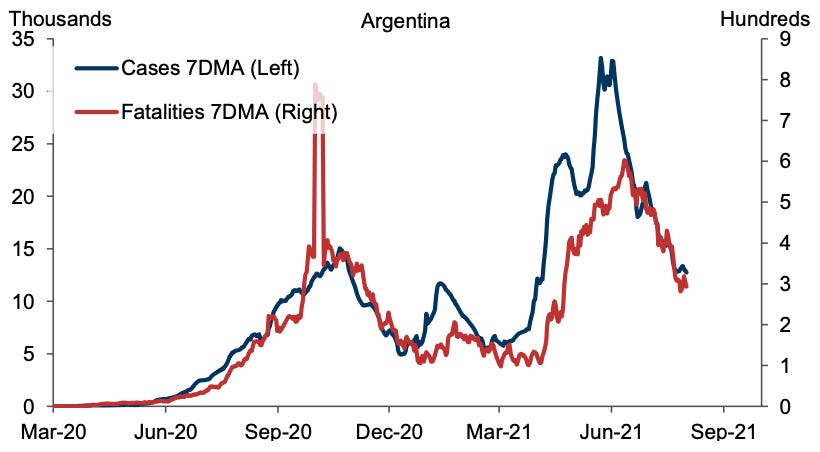
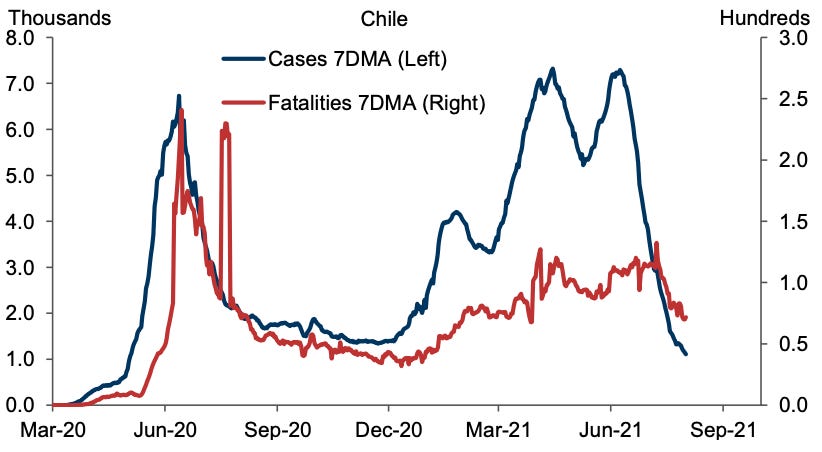
(Note the divergence between cases and fatalities vs. Brazil and Argentina (Goldman Sachs in 2021)).
Overall, the Chinese vaccines are effective, but slightly less so when compared to AZ and J&J’s vaccines. We’re extrapolating for Delta, but assume the same general efficacy until data shows otherwise. Nonetheless, compared to the efficacy rate of a Pfizer or Moderna shot, “pretty good” simply appears to be “not good enough,” especially when everyone else is batting 1.000.
The above does help explain why China is attempting to drive vaccination rates to 100%. It’s all part of a strategy to confer some type of herd immunity for its population. It’s also an attempt to offset the lower efficacy of its vaccines with higher vaccination rates, and number-wise it may work. May. Eventually, we think China will need to offer boosters, or better vaccines to prevent hospitalizations and deaths from overwhelming its healthcare system. Even if we exclude children (i.e., those under 18 and 20% of China’s total 1.4B population), the sheer number of 1.1B adults means that “good enough” may not be enough. The numbers are just too big and patients can quickly overwhelm China’s system.
Still, near-full vaccinations would allow China to reopen borders by the year-end to vaccinated travelers, and slowly and methodically emerge from its current hermit-like state (i.e., similar to Singapore). Meanwhile the healthcare system can also begin deploying booster shots to the populace to further build immunity. For now, we believe the “zero COVID tolerance” policy is a byproduct of lower vaccination rates, but that should begin to fall by the wayside in 2022. China simply needs to dose as many people as possible and as quickly as possible; then keep dosing them to buttress the antibodies already in their systems.
Ultimately, China’s vaccines? Yeah . . surprisingly, they kinda work. I mean, not “fantastically” or “works brilliantly,” but it’s a start, and it’s certainly better than nothing. It’s effectively not much different than dosing the entire country with AZ’s shot, and for a world wracked by a global pandemic, we need all the help we can get.